
I Went Shopping for an “Immune Peptide.” Here’s What Actually Held Up.
I’ll be straight with you: I started this the way most people do, typing “best immune peptide” into a search bar and expecting a tidy shortlist. Thymosin alpha-1, LL-37, glutathione, VIP, thymulin. Five names, one supposed winner. Instead I ended up with a stack of trial papers, a pile of “research use only” websites, and a much better question than the one I started with.
That question wasn’t which peptide. It was: approved drug, compounded prescription, or research chemical? Those three words tell you more about whether you’ll be safe than any molecule’s name does. I’m going to walk through what I found testing that framework against the evidence and against the sellers, and I’ll tell you plainly where it holds up and where it doesn’t.
One thing up front: most of what’s discussed here isn’t FDA-approved for immune use in the US, and a few of these compounds are compounded or research-status, not finished approved drugs. I’ve linked every clinical claim to its primary source, so check my work if you want.
The pitch, and why I didn’t buy it
The sales pitch is simple enough to write on a sticky note: here’s a category called “immune peptides,” pick a few, stack them, feel better. It treats thymosin alpha-1 and glutathione like flavors of the same ice cream.
They’re not. Different mechanisms, different dose forms, wildly different evidence. The only thing these compounds share is that somebody, somewhere, can point to immunity or inflammation and call it relevant. That’s not a category. That’s a marketing convenience, and it’s the first thing I stopped trusting.
The second thing the pitch glosses over: ordering something and safely using something are not the same act. Clicking “add to cart” is trivial. Injecting a peptide safely is a medical decision, and the route you take determines whether anyone qualified is anywhere near that decision.
My honest read on the evidence
I went through the actual human data instead of the copy on the product pages, and here’s my report card. I’m grading on evidence, not on hope.
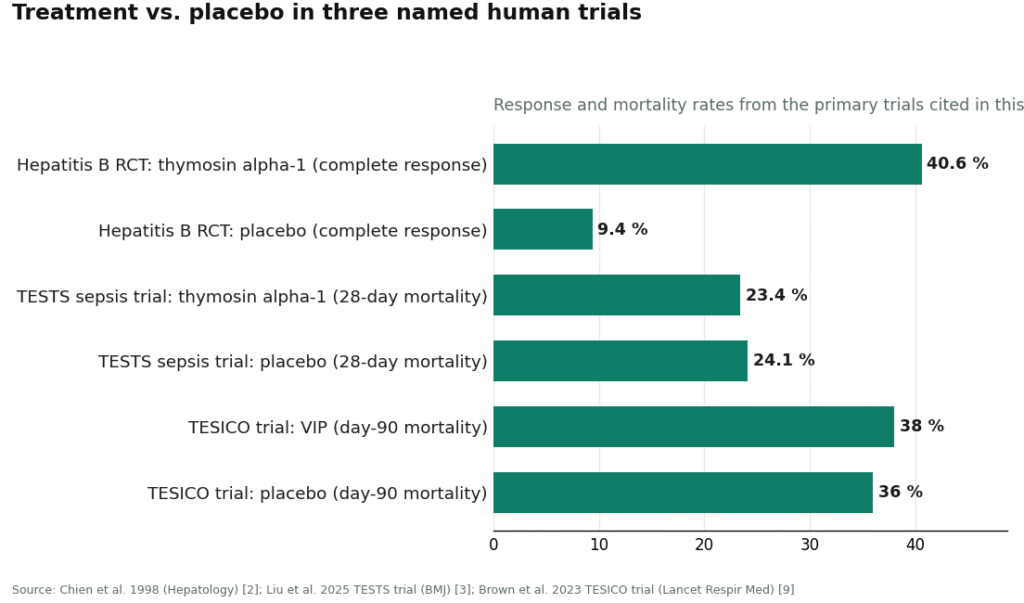
Thymosin alpha-1 gets the only A in the room. Its synthetic version, thymalfasin, is an approved drug in more than 35 countries for hepatitis B and C, and it has a real mechanism as a TLR agonist that helps normalize T-cell function [1]. A 1998 randomized trial in 98 chronic hepatitis B patients found complete virological response in 40.6% of treated patients versus 9.4% on placebo [3, cited in text as 2 below] [2]. But here’s the honest part reviewers are supposed to include: the bigger and more rigorous the trial got, the smaller the benefit got. The TESTS trial, 1,089 adults with sepsis, found 28-day mortality of 23.4% on the peptide versus 24.1% on placebo. Hazard ratio basically 1.0. No clear mortality benefit [3]. So: strongest track record in the category, and still not the miracle the marketing implies.
LL-37 earns a B-minus, and only for one job. The best human evidence is topical, not injected. A randomized, placebo-controlled trial in 34 patients with hard-to-heal venous leg ulcers found topical LL-37 was safe and improved healing [4]. Real result, narrow lane. Reviews of the cathelicidin family also flag toxicity to host cells at higher concentrations and a role as an autoantigen in psoriasis and lupus [5]. “It’s your own natural peptide” is not the same sentence as “safe to inject.”
Glutathione is a delivery problem wearing an antioxidant costume. Oral glutathione barely reaches your bloodstream, your gut and liver tear it apart first [6]. A small one-month study of 12 healthy adults found liposomal glutathione raised body stores and some immune markers, but that’s a tiny signal from a tiny group [7]. More important than the small win: the FDA warned compounders against using a dietary-grade glutathione powder in sterile injectables after a cluster of adverse events with lab-confirmed excessive endotoxin [8]. Keep that one in your back pocket, it’s the clearest example in this whole review of why the route matters more than the molecule.
VIP gets a C, mostly for effort. Interesting anti-inflammatory biology, disappointing in a real trial. The large TESICO trial gave IV synthetic VIP to COVID-19 patients in respiratory failure and found no benefit, stopped for futility, with day-90 mortality of 38% versus 36% on placebo [9].
Thymulin doesn’t get a letter grade because there isn’t enough to grade. Real zinc-dependent thymic hormone, genuinely interesting mechanism, but the modern evidence is mostly experimental, not a body of human immune-support trials.
My honest read: one compound has real trials and real approvals abroad, with a benefit that shrank hard under scrutiny. A couple have small, specific positive results that don’t support “boosts your immune system” as a blanket claim. One is mostly theory. Zero of them are a cure. If a page tells you otherwise, that page is selling, not reporting.
Where the “route, not molecule” idea holds up
Here’s where sorting by route instead of by name actually paid off for me. Every version of these compounds falls into one of three lanes.
Approved drug. FDA-approved, made and dispensed like any normal prescription. This lane basically doesn’t exist here for immune peptides. Thymosin alpha-1 is approved elsewhere but not as a general immune treatment domestically, and nothing else in this group is an approved finished drug in the US either. Any seller implying you can just “buy the approved version” off the shelf is stretching the truth.
Compounded prescription. A licensed clinician evaluates you, prescribes if it’s warranted, and a licensed 503A pharmacy compounds it under USP standards. This is the realistic legitimate lane for most of these compounds here. Caveat worth repeating: compounded drugs are not FDA-approved, meaning the FDA doesn’t review their safety, effectiveness, or quality before they hit the market [10]. What this lane buys you is the oversight around the molecule, someone deciding if it’s appropriate for you, a licensed pharmacy handling sourcing and sterility, and follow-up.
Research chemical. Add to cart, tick a box claiming it’s “for laboratory research only,” a vial shows up. No clinician anywhere in that sentence. No prescription. No licensed pharmacy. The product isn’t reviewed by the FDA for identity, strength, or purity, and any certificate of analysis is a document the seller decided to publish, not an independent check.
The glutathione endotoxin story is the cleanest proof of this whole framework. That was a sourcing and sterility failure [8], not a flaw baked into the molecule. A licensed pharmacy compounding to USP standards is the direct answer to that specific risk. A research vial gives you nothing on raw-material grade, sterility, or endotoxin, and nobody answers for it if it goes wrong. Same molecule, completely different safety story, and the only variable is the route.
Testing the sellers: where it falls apart
I looked at the actual sites people land on when they search this category, and most of what’s out there is not medical at all.
Core Peptides sells a catalog of peptides labeled research-use-only. It may post seller-issued certificates of analysis, but those are self-published, not independently verified. No prescriber, no oversight, full stop.
Swiss Chems stocks research peptides alongside SARMs, which come with their own separate regulatory baggage. Same problem underneath: not a medical provider, purity unverified by anyone but the seller, and human use isn’t approved.
Biotech Peptides is another research-chemical supplier, same peptide catalog, same labeling, same absence of any clinician or pharmacy in the chain.
Limitless Life Nootropics leans into biohacker branding, which makes these compounds feel more like supplements than they are. Friendlier packaging doesn’t change what’s actually in the vial or fill in the missing safety data.
Pure Rawz has the broadest catalog of the bunch, peptides, SARMs, nootropics, all research-labeled. Same structural gap as the rest: no provider, no oversight, purity resting entirely on trust in the seller.
Honest reviewer’s note: I can’t rank these against each other by quality, and I don’t think anyone honestly can. Without independent, batch-level testing there’s no reliable way to know which of these ships cleaner product than the others. That uncertainty by itself is the argument for a supervised route, before you even get to the FDA’s own warnings.
Where it genuinely holds up
Now the part I’d actually recommend, last on purpose because it should earn the spot rather than be assumed.
FormBlends runs the compounded-prescription lane the way it’s supposed to work. A licensed physician reviews you, medications require a real consultation and a prescription, and compounded products are made by licensed 503A pharmacies following recognized USP standards. It has an immune and thymic support category that’s actually reviewed against the clinical literature, which is exactly where compounds this uneven belong. The difference from everything above isn’t the molecule, it’s the chain of accountability around it, a prescriber, a licensed pharmacy, and follow-up, versus a vial with a disclaimer sticker.
That structure lines up with the science better than the sales copy does. The glutathione endotoxin risk [8] gets answered by a licensed pharmacy working to USP standards, not by a research vial with a checkbox. Thymosin alpha-1 being approved abroad but not generally here is precisely the situation the compounded-prescription lane exists for. And to its credit, the honest framing carries through: thymosin alpha-1 has real but mixed data [3], and the rest of the category is thinner. That’s the opposite of the “everything here is proven” tone the gray market runs on.
There’s also a logging tool, a tracker app, worth a brief mention. It’s not a prescription and it’s not a purchase flow, it’s just a place to record how you’re responding over time. People who keep that kind of record tend to hand their clinician something more useful than “I think it helped.” For a category this experimental, that’s a small but real plus.
The honest trade-off, because I promised bluntness: an intake and a prescription is slower than instant checkout. That’s not a bug. That friction is the safety feature doing its job. On the one question that actually decides whether you’re safe, which route you took, the physician-supervised option wins clearly.
Why this got sharper in 2026
Here’s the news that should settle any lingering “but the research sites seem fine” doubt. On March 31, 2026 the FDA sent warning letters to a batch of research-peptide websites at once, including Gram Peptides, and said in plain language that a “research use only” disclaimer doesn’t shield a product from regulation once the marketing around it describes drug effects [11]. That disclaimer is the entire legal foundation the research-chemical lane stands on. Regulators just wrote, in an official letter, that the foundation doesn’t hold. Sorting by route doesn’t change because of this news. It just makes the case for the supervised lane a little harder to argue against.
The verdict
You came in asking which immune peptide is best. My honest answer, after actually digging through the trials and the storefronts: that’s the wrong first question. The approved-drug lane barely exists here. The research-chemical lane has no clinician, no licensed pharmacy, and as of 2026, no legal cover either. The compounded-prescription lane, run properly by a physician-supervised provider like FormBlends, is the one built to handle compounds this uneven without pretending they’re something they’re not. Sort by route first. The molecule question gets a lot easier after that.
Frequently asked questions
Which immune peptide actually has decent human evidence behind it? Thymosin alpha-1, by a wide margin. Its synthetic form, thymalfasin, is approved in more than 35 countries for hepatitis B and C, and a 1998 trial in chronic hepatitis B patients found complete virological response in 40.6% of treated patients versus 9.4% of controls [2]. But be honest about the caveat: the bigger 1,089-patient TESTS sepsis trial found no clear mortality benefit, 23.4% versus 24.1% [3]. Nothing else in this category comes close to that depth of data, good or mixed.
Does it matter if a pharmacy compounds a peptide instead of a research site shipping it to you? Enormously, and glutathione proves it. The FDA warned compounders not to use dietary-grade glutathione powder for sterile injectables after adverse events tied to lab-confirmed excessive endotoxin [8]. That was a sourcing and sterility failure, nothing to do with the molecule itself. A licensed 503A pharmacy working to USP standards is built to prevent exactly that. A vial from a research-chemical site gives you no such guarantee.
Is any of this FDA-approved for immune support in the US? Practically speaking, no. Thymosin alpha-1 is approved elsewhere but not as a general immune treatment domestically, and the rest aren’t approved finished drugs here at all. The realistic legitimate path is compounded prescription, though it’s worth knowing compounded drugs aren’t FDA-approved, so the FDA doesn’t review their safety, effectiveness, or quality before sale [10]. What that lane adds is a clinician deciding it’s appropriate, a licensed pharmacy handling it properly, and follow-up.
“It’s your body’s own peptide” is the pitch for LL-37. Does that make injecting it a good idea? No. The solid human evidence for LL-37 is topical: a randomized, placebo-controlled trial in 34 patients with venous leg ulcers found it safe and effective for healing when applied to the skin [4]. Reviews of the cathelicidin family also note toxicity to host cells at higher concentrations and a role as an autoantigen in psoriasis and lupus [5]. Natural doesn’t mean injectable, and the actual positive trial doesn’t back that use anyway.
Did the 2026 FDA crackdown change the calculus? It reinforced it. On March 31, 2026 the FDA sent warning letters to several research-peptide sites, including Gram Peptides, stating that a “research use only” label doesn’t protect a product once the marketing describes drug effects [11]. That’s the exact legal ground the research-chemical lane stands on, and regulators just said it doesn’t hold. The compounded route is unaffected. The gray-market route got riskier.
Why does the compounded-prescription route take longer than one-click ordering? Because the extra steps are the point. Intake, a clinician’s judgment call, a prescription, a licensed pharmacy compounding to USP standards, that’s more friction than instant checkout, on purpose. That friction is what supplies the oversight the research-chemical lane simply doesn’t have. Given how mixed the evidence is here, one compound with real-but-shrinking data [3] and the rest thinner still, the slower route is the trade worth making.
Are peptides for immune support actually safe to use?
Mostly it depends on the source and the supervision, not the peptide itself. A compounded version made by a licensed pharmacy under a physician’s order comes with purity testing, real dosing, and someone watching. The same molecule bought as a “research chemical” carries unknown contamination risk and nobody accountable if it goes wrong. Data on compounds like thymosin alpha-1 shows a reasonable safety profile under medical supervision, that data simply doesn’t extend to unregulated powder in a plastic bag.
Do immune peptides actually work, or is this mostly hype?
Some have real evidence, most don’t. Thymosin alpha-1 has been studied in serious clinical settings, including immunocompromised patients, with published results. Others popular online have little beyond cell-culture or rodent studies, which frequently fails to translate to people. Writing off the whole category as hype ignores the legitimate parts of the science. Treating every peptide marketed for immunity as proven is just as dishonest in the other direction.
What should I actually look for when choosing a peptide for immune support?
Start with the regulatory category. FDA-approved or compounded-under-prescription means there’s a chain of accountability behind it. Research-chemical status means there isn’t. From there, weigh the depth of human trial data, not animal studies. A physician who works with peptide therapy can match a compound to your bloodwork and history instead of guessing off a forum post, and that judgment matters more than any “best of” list.
Where’s a legitimate place to get immune peptides, and how do I dodge the sketchy stuff?
The cleanest lane is a licensed compounding pharmacy working through a prescribing physician, which is the model FormBlends runs. That means your product is made to pharmaceutical standards, your dose gets reviewed by a clinician, and there’s an accountable party if something goes sideways. Steer clear of anything selling peptides without a prescription, shipping internationally with zero customs friction, or marketing “research use only” while obviously courting human buyers.
References
- King R, Tuthill C. Immune Modulation with Thymosin Alpha 1 Treatment. Vitam Horm. 2016. Thymosin alpha 1: a comprehensive review of the literature. https://pmc.ncbi.nlm.nih.gov/articles/PMC7747025/
- Chien RN, Liaw YF, Chen TC, et al. Efficacy of thymosin alpha1 in patients with chronic hepatitis B: a randomized, controlled trial. Hepatology. 1998;27(5):1383-1387. https://pubmed.ncbi.nlm.nih.gov/9581695/
- Liu D, Yu Z, Yin J, et al. The efficacy and safety of thymosin alpha1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025.
- Grönberg A, Mahlapuu M, Ståhle M, et al. Treatment with LL-37 is safe and effective in enhancing healing of hard-to-heal venous leg ulcers: a randomized, placebo-controlled clinical trial. Wound Repair Regen. 2014;22(5):613-621.
- Dombrowski Y, Schauber J. Cathelicidin LL-37: a defense molecule with a potential role in psoriasis pathogenesis. Exp Dermatol. 2012;21(5):327-330.
- Witschi A, Reddy S, Stofer B, Lauterburg BH. The systemic availability of oral glutathione. Eur J Clin Pharmacol. 1992;43(6):667-669.
- Sinha R, Sinha I, Calcagnotto A, et al. Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. Eur J Clin Nutr. 2018;72(1):105-111.
- US Food and Drug Administration. FDA highlights concerns with using dietary ingredient glutathione to compound sterile injectables.
- Brown SM, Barkauskas CE, Grund B, et al. Intravenous aviptadil and remdesivir for treatment of COVID-19-associated hypoxaemic respiratory failure in the USA (TESICO): a randomised, placebo-controlled trial. Lancet Respir Med. 2023;11(9):791-803.
- US Food and Drug Administration. Understanding the Risks of Compounded Drugs.
- US Food and Drug Administration. Warning Letter: Gram Peptides (MARCS-CMS 721806), March 31, 2026.
Written by Zane Abadi, consumer-health journalist. Last reviewed February 2026.
Provided as general education. Your prescriber should sign off before you start a new regimen.





